
The inevitability of infection
The end of Zero Covid, the tripledemic, and first contact with the New World

As China exits from Zero Covid, there are projections that as many as one million Chinese people will die in the coming months. (I should say more properly that there is one projection that has been extensively reported on. I don’t want to parrot and exaggerate a preprint title, but the exact number isn’t important.)
China’s Zero Covid policy has prevented hundreds of millions of Covid-19 infections, which is admirable. But there have been two major downsides. The first is the tremendous damage that draconian Zero Covid policies have done in terms of healthcare, emergency response, the economy, and quality of life. The second downside is the lack of an endgame.
Zero Covid would have been a good policy on its own if Covid-19 had died out quickly and gone functionally extinct. Most Chinese people would have been protected from the disease, and that would be that. Zero Covid would also have made sense as an acute response measure, a way to buy time to vaccinate the population and prepare for the eventual exit from Zero Covid.
Instead, the exit from Zero Covid seems haphazard. The Chinese population is not as well-vaccinated as it should be, and a sudden exit will lead to a spike in infections, which leads to overwhelmed hospitals, which leads to people suffering or dying from illnesses or injuries that they wouldn’t have suffered or died from if hospitals weren’t overwhelmed.
It didn’t have to be this way, with a million deaths from the exit. With tools like vaccination and phased reopening, many lives could have been saved, not because people would never be infected, but because they would be vaccinated and then infected, or because they might get infected next year rather than this year, or because they would end up in a hospital ready to treat them rather than in a hospital where desperate patients are lining the hallways.

Pathogens and parasites have existed for about as long as life itself, and for as long as there have been humans, there have been human diseases. As humans arose in Africa a few million years ago, they were already in a soup of pathogens and parasites that were adapted and ready to infect them. So it might seem that, from the point of view of infectious diseases, there never was a golden age of savage nobility.
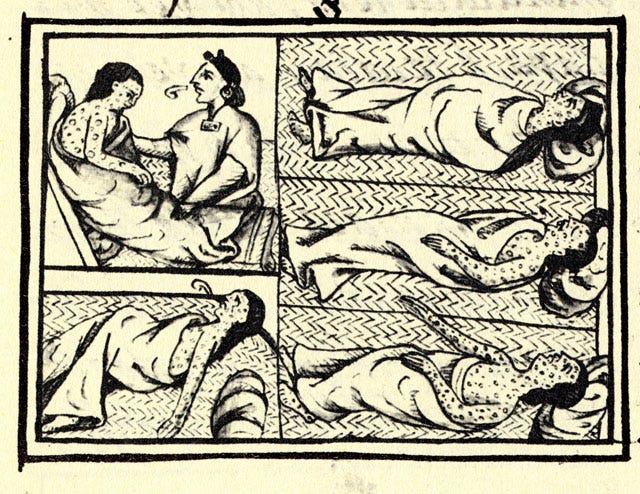
But in fact, something like this probably happened when European explorers came to the Americas. In these first encounters, neither side knew what to make of the other. Language was obviously a problem, and the difference in skin colors and physiognomy was likely notable.
But there was another layer: disease. The Europeans were probably, to our modern eyes, in a sorry state: short because of poor childhood nutrition, with pockmarked skin from infections like smallpox and chickenpox. The Indians, on the other hand, especially the nobles, were striking and handsome, tall and smooth-skinned. They ate well and, perhaps surprisingly to the Europeans, did not suffer from many diseases.

(I understand that many of my readers probably object to the term “Indians” and would prefer “Indigenous.” My understanding –which I would sincerely appreciate having corrected– is that the change in nomenclature, from “Indian” to “Native American” to “Indigenous,” is a product of white people’s difficulty in developing terminology to collectively refer to people that don’t have much of a reason to be in a collection except for white people’s need to have them in a collection. The most salient overlap between the Taíno, Hawaiians, and Inuit is not linguistic or cultural; it is that they were oppressed by European colonists. It should not be surprising that these disparate people do not have a clear consensus of what they would like white people to call them. Thus, I use the term “Indian” here not to disrespect these many different peoples, nor to cast aspersions on efforts to best reconcile our current situation with sins of the past, but instead to draw attention to the fact that many Indigenous people –again, as I understand it– don’t really like that name and really would prefer “Indian.”)
There are a few reasons that one population might suffer fewer infectious diseases than another. Clean water, sewer systems, and wastewater treatment prevent the transmission of diseases that are transferred through human feces, like typhoid, cholera, and tapeworms. Vaccines can prevent or reduce the transmission of diseases like measles, chickenpox, and polio.
But the reason for the relative dearth of infectious diseases among pre-contact humans in the Americans wasn’t wastewater treatment or vaccines. The reason was quarantine. As humans left Africa, they initially carried many pathogens with them. But through time and across the distance traveled, fewer and fewer stayed with them. Pathogens that relied on mosquitoes for transmission couldn’t follow where there were no mosquitoes. And if some group of people simply didn’t carry a pathogen with them when they left from other humans in Africa and Asia and moved further into the Americas, then that simply didn’t come along. If no one who made it across the Bering Strait land bridge had measles, then there would be no measles in the Americas.
New pathogens can always arise, but most new, human-infecting pathogens are bacteria or viruses that were already adapted to humans or similar hosts, like pigs or chickens. The humans that first traveled to the Americas simply didn’t bring enough of the raw material needed for the kinds of infectious disease burden that was in Africa and Europe.
While this situation of limited infectious diseases lasted, it was a good thing. Between when the Bering Strait land bridge was covered up, around 20,000 years ago, and when Europeans crossed the Atlantic in 1492, the Old World and New World were essentially two enormous “pods.” If, during some part of the Covid-19 pandemic, you lived in a house with a small number of other people and really never went anywhere or got close to anyone else, then voilà, you never had any chances to catch any diseases. And the same was true of the people in the Americas: they simply didn’t have any way to catch any of the diseases their ancestors had left behind, or that had newly arisen in the Old World.
But just as the breakup of the Covid pods meant catching all sorts of infectious diseases, all the many sniffles and coughs and stomach bugs we had forgotten about and lived without, so contact between the New and Old Worlds meant an exchange of pathogens. This exchange was mostly one way, because the “raw material” for human-infecting pathogens was mostly in the Old World, with its ancestral pathogens and many intermediate hosts. It’s possible that a few American diseases made their way back to Europe, but for the most part, it was European diseases that came to the Americas.
{kind=link}
Their impact of those diseases on the people in the Americas was, with no exaggeration, apocalyptic. It’s estimated that as much as 90% of the people in the Americas were killed by infectious diseases imported from Europe. There is substantial debate over what drove this death rate, whether it was simply lack of immunity or if it was a combination of other kinds of marginalization and brutalization by colonizers that made the native Americans more susceptible to disease.
Enslavement and direct violence killed huge proportions of the populations that were in direct contact with Europeans, but it seems that, when Europeans arrived in a new area, the locals were already in a bad way. The picture I have is that European diseases spread ahead of the Europeans themselves, and when Europeans actually arrived, they found societies devastated by unthinkably destructive epidemics.
Deaths due to enslavement and direct violence could have been prevented if the European colonizers were not racist and violent. Deaths due to a combination of oppression and infectious disease could also have been prevented. But deaths to infectious disease per se would have happened, one way or another.
The only solutions, as far as I understand, would be continued quarantine of the American continents, or mass vaccination of the entire population of the Americas. Both seem far-fetched.
This winter’s “tripledemic” of Covid-19, influenza, and RSV seems to be mostly a matter of pod-exiting. The Delta and Omicron waves were driven primarily by new, more contagious Covid-19 variants, but I don’t think there is evidence that strains of RSV or influenza virus circulating this year are meaningfully more infectious than strains circulating in previous years. Instead, it’s like we’re getting a larger-than-average flu season, and a double-size RSV season, and another Covid winter, all at the same time.
With RSV in particular, we tend to naturally “flatten the curve.” Only one generation of newborn children gets infected with RSV each year, producing immunity among those children. By the time next winter comes, there is only one years’ worth of new children who are mostly susceptible. This year, we have lower than average population-wide immunity to the flu, and we have multiple years’ worth of children who are RSV-susceptible, all because of our years of quarantine and reduced contact. It’s the pain of the Covid pod-exiting, just at a population scale.
While infection with endemic diseases might be inevitable, it doesn’t mean things are hopeless. Vaccines are a marvel and the closest thing you will get to a Marvel superpower. The flu and Covid-19 vaccines substantially reduce the chances that an infection will lead to hospitalization or death. Improving air ventilation and filtration has huge benefits for reducing transmission of most respiratory diseases. You should protect yourself and your community, and flatten the curve. Even if you’ll get the flu someday, if you can stave it off for one more year, that’s a bit more of a chance that someone who needs that hospital bed for another reason can get it.
When Europeans came to the Americas, there was no option to vaccinate everyone against the new diseases. But there was a better way to do China’s exit from Zero Covid. Today, the inevitability of infection need not equate to fatalism.
Well personally I love history and I'm a microbiologist by profession, so more at the intersection of those two things would suit me!
And while it's a bit morbid, I guess the epidemiologist part of me (which is quite small) is interested in the Old World/New World disease exchange. We think of some of the Old World diseases as having developed there because of higher population densities etc (although the bubble effects/bottleneck you spoke about will undoubtedly have had a big impact too). Did the lower population densities in modern day US/Canada affect which of the Old World diseases were "successful"?
Nice post! Tiny thing - I think you meant typhoid not typhus? Typhus is spread by insects, not faeces?